In recent years, significant progress has been made in the clinical treatment of hepatocellular carcinoma. SHARP is the first clinical trial to lay the foundation for the use of multi-target receptor tyrosine kinase inhibitors (RTKI) for the treatment of liver cancer, which has achieved 5 successful Phase 3 clinical trials.
The Phase 2 clinical trials of PD1 inhibitors nivolumab and pembrolizumab showed good prospects and led to accelerated approval by the FDA. The latest Phase 3 clinical trials showed that the anti-PD-L1 antibody atezolizumab and the anti-VEGF antibody bevacizumab (atezo/bev) as a first-line combination therapy are stronger than sorafenib, with superior progression-free survival (PFS) and overall survival (OS). This is the first clinical trial to achieve this goal since SHARP. Therefore, atezo/bev (atezolizumab + bevacizumab) has now become the new standard for the first-line treatment of advanced HCC, and all upcoming clinical trials need to be tested according to this new benchmark.
First-line and second-line systemic treatment of advanced liver cancer
Several treatments are trying to follow the footsteps of atezo/bev.
* Cabozantinib combined with atezolizumab
* Lenvatinib combined with pembrolizumab
* Durvalumab combined with anti-CTLA-4 antibody tremelimumab
* Nivolumab combined with ipilimumab
* Anti-PD-1 antibody camrelizumab combined with apatinib and anti-PD-1 antibody tislelizumab as a monotherapy.
These combined therapies are currently undergoing Phase 3 clinical trials, using the same similar design that all trials are first-line treatment, including patients with unresectable HCC, that is, mid-stage patients (BCLC B), and advanced patients (BCLC C). The only exception is nivolumab combined with ipilimumab, which is limited to advanced HCC.
Systemic treatment of mid-stage liver cancer
The IMbrave 150 trial included patients with unresectable HCC, namely BCLC B and C stages, of which 80% of patients were in BCLC C stage. As the proportion of BCLC stage B patients is quite small (~15%), it is currently impossible to finalize the efficacy of atezo/bev in this type of patient group, especially when compared with transcatheter arterial chemoembolization (TACE) treatment.
ABC-HCC is a large Phase 3b clinical trial comparing atezo/bev and TACE. In addition, RENOTACE is another large Phase 3 clinical trial that will test the effect of regorafenib combined with nivolumab compared with TACE. These two clinical trials will pave the way for systemic treatment of BCLC stage B patients.
Another approach to treating mid-stage liver cancer is to add systemic therapy to TACE. There are currently three Phase 3 trials in progress. LEAP-012 is testing the addition of lenvatinib and pembrolizumab to TACE. In EMERALD-1 trial durvalumab or durvalumab plus bevacizumab is added to TACE, In the CheckMate 74W trial nivolumab or nivolumab plus ipilimumab is added to TACE. Each of these tests will be compared with TACE individually.
Adjuvant therapy
So far, no systemic treatment has been proven to be beneficial in the adjuvant treatment of therapeutic hepatectomy or ablation.
Four ongoing Phase 3 trials are exploring new methods.
CheckMate 9DX trial is testing adjuvant therapy with nivolumab.
KEYNOTE-937 trial is testing adjuvant therapy with pembrolizumab.
IMbrave050 trial tests atezolizumab and bevacizumab adjuvant therapy.
EMERALD-2 trial tests the adjuvant therapy of durvalumab with or without bevacizuma.
Neoadjuvant therapy
There are currently no mature data to support the use of systemic drugs before surgery or local treatment. However, early clinical trials evaluating neoadjuvant therapies are underway. The NIVOLEP trial is evaluating the efficacy of nivolumab before and after electroporation ablation. The CaboNivo trial is evaluating the safety of combining cabozantinib and nivolumab before locally advanced/borderly resectable HCC hepatectomy.
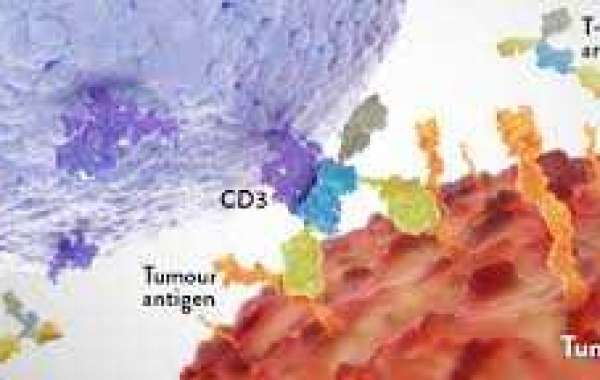
Cell therapy and gene therapy
Most of the cell and gene therapies of HCC are still in the preclinical or early clinical stage. Such immunotherapies include chimeric antigen receptor (CAR) T cells, allogeneic NK cells, and oncolytic viruses.
In recent years, systemic treatment of liver cancer has made considerable progress. So far, atezo/bev is the first and only immunotherapy effective against liver cancer. Such drugs are no longer limited to advanced HCC, but include the early stages of the disease. In addition, other immunotherapy methods, such as CAR-T or CAR-NK cells, have now entered the clinical development stage, and may further expand the scope of treatment for HCC.